According to the NCCN
Guidelines®, testing for measurable residual disease (MRD) first requires a bone marrow
sample.1 The highest-quality sample comes from the first or an early pull, to avoid
hemodilution.2 The first small volume (up to 3 mL) pull of a bone marrow aspirate is preferred.1 The second pull has shown an approximately 50% reduction in
leukemic cells.2 When a bone marrow sample cannot be acquired, peripheral blood may be used
as an alternative sample when high-sensitivity methods for quantification are used; however, note that
the use of bone marrow is preferred.3
Watch Aaron Logan discuss the importance of the first bone marrow aspirate pull
Aaron Logan, MD, PhD
Associate Professor of Clinical Medicine The University of California, San Francisco
MRD can be quantified by various methods, with sensitivity thresholds ranging from
< 1 × 10-4 (< 0.01%) to < 1 x 10-6 (
< 0.0001%).1 Consider consulting with a pathologist prior to
testing for considerations that may yield the best results.
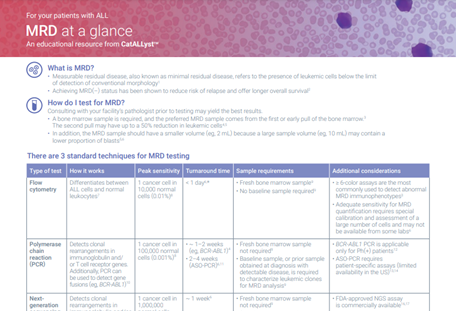
There are 3 common techniques used to quantify MRD:1
Type of test
Flow cytometry
Quantitative polymerase chain reaction (Q-PCR)*
Next-generation sequencing (NGS)
Target
Leukemia-associated immunophenotypes4
Immunoglobulin/T-cell receptor gene rearrangements or gene fusions (eg,
BCR-ABL1)5
1 cancer cell in 1,000,000 normal cells (0.0001%)6
Turnaround time
~ 1 day4,5
~ 1–2 weeks (eg, BCR-ABL1)7
3–4 weeks for diagnostic
sample, ~ 1 week for follow-up
analyses (ASO-PCR)8
~ 1 week4
Sample requirements
Fresh sample6
Baseline sample preferred but not required6,‡
Requires baseline sample, or prior sample obtained at diagnosis with detectable
disease6
Requires baseline sample, or prior sample obtained at diagnosis
with
detectable disease6
Additional considerations
Adequate sensitivity for MRD quantification requires special calibration and
assessment of a large number of cells and may not be available from some
labs8
Requires significant
expertise for analysis6
Limited standardization across testing facilities6
BCR-ABL1 PCR is applicable
only in Ph(+) patients9
ASO-PCR utilizes
patient-specific ASO primers (limited availability in the US)9
Limited standardization across testing facilities, depending
on assay6
FDA-cleared NGS assay available6
Limited standardization across testing facilities using other NGS approaches6
Type of test
Flow cytometry
Target
Leukemia-associated immunophenotypes4
Typical sensitivity†
1 cancer cell in 10,000 normal cells (0.01%)6
Turnaround time
~ 1 day4,5
Sample requirements
Fresh sample6
Baseline sample preferred but not required6,‡
Additional considerations
Adequate sensitivity for MRD quantification requires special calibration and
assessment of a large number of cells and may not be available from some
labs8
Requires significant
expertise for analysis6
Limited standardization across testing facilities6
Type of test
Quantitative polymerase chain reaction (Q-PCR)*
Target
Immunoglobulin/T-cell receptor gene rearrangements or gene fusions (eg,
BCR-ABL1)5
Typical sensitivity†
1 cancer cell in 100,000 normal cells (0.001%)6
Turnaround time
~ 1–2 weeks (eg, BCR-ABL1)7
3–4 weeks for diagnostic
sample, ~ 1 week for follow-up
analyses (ASO-PCR)8
Sample requirements
Requires baseline sample, or prior sample obtained at diagnosis with detectable
disease6
Additional considerations
BCR-ABL1 PCR is applicable
only in Ph(+) patients9
ASO-PCR utilizes
patient-specific ASO primers (limited availability in the US)9
Limited standardization across testing facilities, depending
on assay6
1 cancer cell in 1,000,000 normal cells (0.0001%)6
Turnaround time
~ 1 week4
Sample requirements
Requires baseline sample, or prior sample obtained at diagnosis
with
detectable disease6
Additional considerations
FDA-cleared NGS assay available6
Limited standardization across testing facilities using other NGS approaches6
Guideline
recommendations for when to test for MRD
Guideline recommendations for when to test for MRD
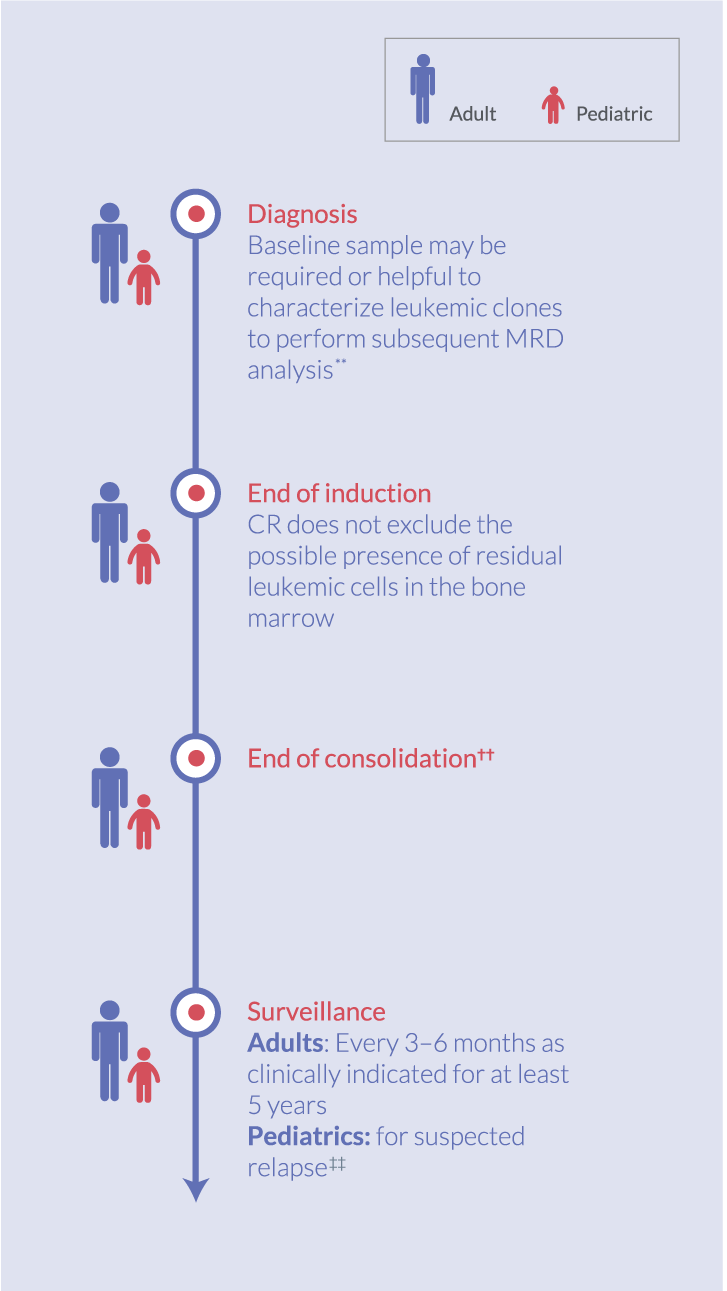
NCCN Guidelines state that testing for measurable residual disease (MRD) is an essential component of patient evaluation over the course of sequential therapy in pediatric and adult patients with ALL.1,10 The guidelines recommend characterization of leukemic clones at diagnosis for subsequent MRD testing when using some techniques, MRD testing upon completion of initial induction therapy and at the end of consolidation therapy, and subsequent testing at various time points throughout a patient’s treatment journey.1,10
MRD testing timeline1,10,§
Diagnosis
Baseline sample may be
required or helpful to
characterize leukemic clones
to perform subsequent
MRD analysis**
End of induction
CR does not exclude the
possible presence of
residual leukemic cells in
the bone marrow
End of consolidation††
Surveillance
Adults: Every 3–6 months
as clinically indicated for at
least 5 years Pediatrics: for suspected
relapse‡‡
MRD status plays an important role in a patient’s treatment journey, and an MRD(+) test result may prompt additional intervention or a change in treatment1,10
Aaron Logan discusses the MRD testing methods:
Aaron Logan, MD, PhD
Associate Professor of Clinical Medicine The University of California, San Francisco
James McCloskey shares his perspective on when to test for MRD:
James McCloskey, MD
Interim Chief, Division of Leukemia The John Theurer Cancer Center
Where can
I test for MRD?
Where can
I test for MRD?
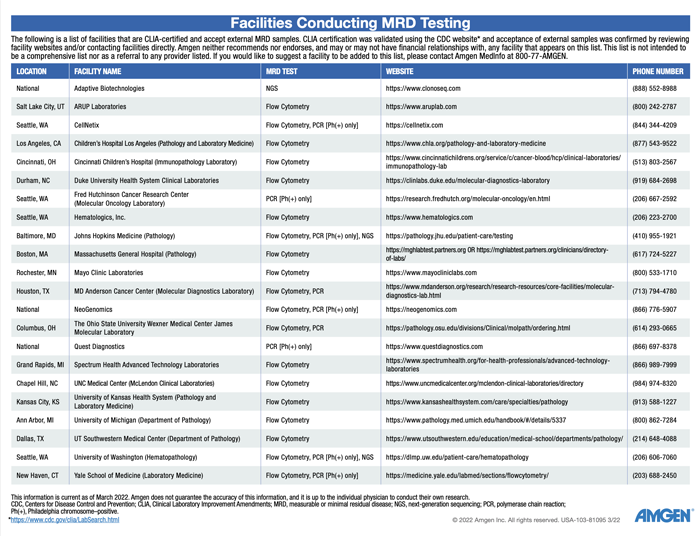
The measurable residual disease (MRD) test can be performed in-house at some institutions, or the sample can
be sent to an outside laboratory if necessary.11 You can speak with your pathologist
first, as they may have some input or experience with how and where to test.
MRD
pathology reports: helpful perspectives
MRD pathology reports: helpful perspectives
Useful information to include in an MRD pathology
report based on the clinical experience of the opinion leaders brought together by Amgen Oncology
The following information could be useful to include in a measurable residual disease (MRD) pathology report:
Relevant patient information, such as patient name, date of birth, medical history, treatment history
(eg, prior CD19- or CD22-targeted therapy), and current treatments (eg, treatment phase, cycle of
therapy, day of therapy), to ensure communication of all patient-relevant information between the
hematologist/oncologist and pathologist5,12,13
A topline summary of results on the front page of the report for easy accessibility
Sample information (eg, type/source, adequacy, reasons if needed/when appropriate why it is not optimal,
if applicable), assay details (eg, methodology, assay sensitivity, number of cells assayed), and any
associated limitations, to assist the treating oncologist in making informed treatment decisions based
on MRD test results6,7,14,15
MRD results summary, a concise summary on residual cells detected to help guide the treating oncologist
in determining next steps in the patient’s treatment journey15
MRD results over time, to provide a snapshot of the patient’s MRD status over the course of
treatment15
Interpretation of MRD test results
You may consider the following, based on the clinical experience of the opinion leaders brought together by
Amgen Oncology:
Interpretation of measurable residual disease (MRD) results may be influenced by the maximum sensitivity
of the test being used14
False-negative and false-positive results are possible, based on the test being used14
Results are usually reported as the number (percentage) of blasts in a sample15,16
An MRD(+) test result may warrant additional intervention or a change in treatment1,10
Continue to monitor the patient’s MRD status following an MRD(–) test result, as clinically
appropriate1,9
Brent Wood and Aaron Logan discuss more in-depth considerations for the MRD pathology report, from template creation to interpretation of results:
Brent Wood, MD, PhD
Professor of Laboratory Medicine Children’s Hospital Los Angeles
Aaron Logan, MD, PhD
Associate Professor of Clinical Medicine The University of California, San Francisco
MRD sample journey
The measurable residual disease (MRD) testing journey involves several steps that require multidisciplinary
communication among the ordering hematologist/oncologist, the pathologist, and the testing facility—from
ordering an MRD test to processing and handling samples, reporting and interpreting test results, and
determining the next steps in the treatment journey.12,17
Jae Park discusses more in-depth considerations for MRD in ALL, including an MRD sample journey:
Jae Park, MD
Associate Attending Physician Memorial Sloan Kettering Cancer Center
Collaborating with your multidisciplinary team
ensures optimal results in MRD
assessment12,17
MRD resources
for you and your practice
MRD resources for you and your practice
Download MRD at a glance
A resource containing practical information on implementing MRD testing in your practice
Download the MRD testing facilities list
A list of facilities that test for MRD, if you are looking to test
at an outside center
Download the sample pathology report presentation
A sample pathology report presentation that highlights considerations and best practices for
MRD pathology report template creation, reporting, and interpretation of results
Download the MRD methodologies presentation
From ordering an MRD test to interpreting the results, this
resource illustrates MRD considerations throughout the testing journey
†Assays with < 0.01% sensitivity cannot be used to quantify MRD accurately.5
‡For different-from-normal (DfN) method only.6
§AYA patients can be included in either pediatric or adult patient populations.1,10
**Dependent on MRD testing technique used.1,10
††Additional time points should be guided by the regimen used. Serial monitoring frequency may be increased in patients with molecular relapse or persistent low-level disease burden.1,10
‡‡MRD testing may be included with a bone marrow
aspirate.10
ALL, acute lymphoblastic leukemia; ASO, allele-specific oligonucleotides; AYA, adolescent and young adult; BCR-ABL1, breakpoint cluster region protein-abelson murine leukemia viral oncogene homolog 1; CD, cluster of differentiation; CR, complete remission; MRD, measurable residual disease; NCCN, National Comprehensive Cancer Network; NGS, next-generation sequencing; PCR, polymerase chain reaction; Ph(+), Philadelphia chromosome–positive; Q-PCR, quantitative PCR.
 How
do I
test for
How
do I
test for